You have received a diagnosis of keratoconus, and ever since you have been reading online and feeling frightened. Perhaps it is you, and perhaps it is a teenage son or daughter about whom, at a routine eye examination, you suddenly heard a word you had never come across. And almost everywhere you look, the message is the same: you have keratoconus, you need cross-linking, and quickly. I want to do something different here — to explain calmly what this condition really is, and why the diagnosis alone does not yet mean you need surgery. For some people cross-linking really is the right and urgent treatment; for others the right thing is in fact structured monitoring. The difference between the two is the whole point, and it is exactly what good diagnosis is meant to determine.
On this page I will explain what happens in the cornea in keratoconus, what cross-linking does and does not do, who needs it and when, and how vision is corrected — which, as we shall see, is an entirely separate story from treating the cornea itself.
What Keratoconus Is
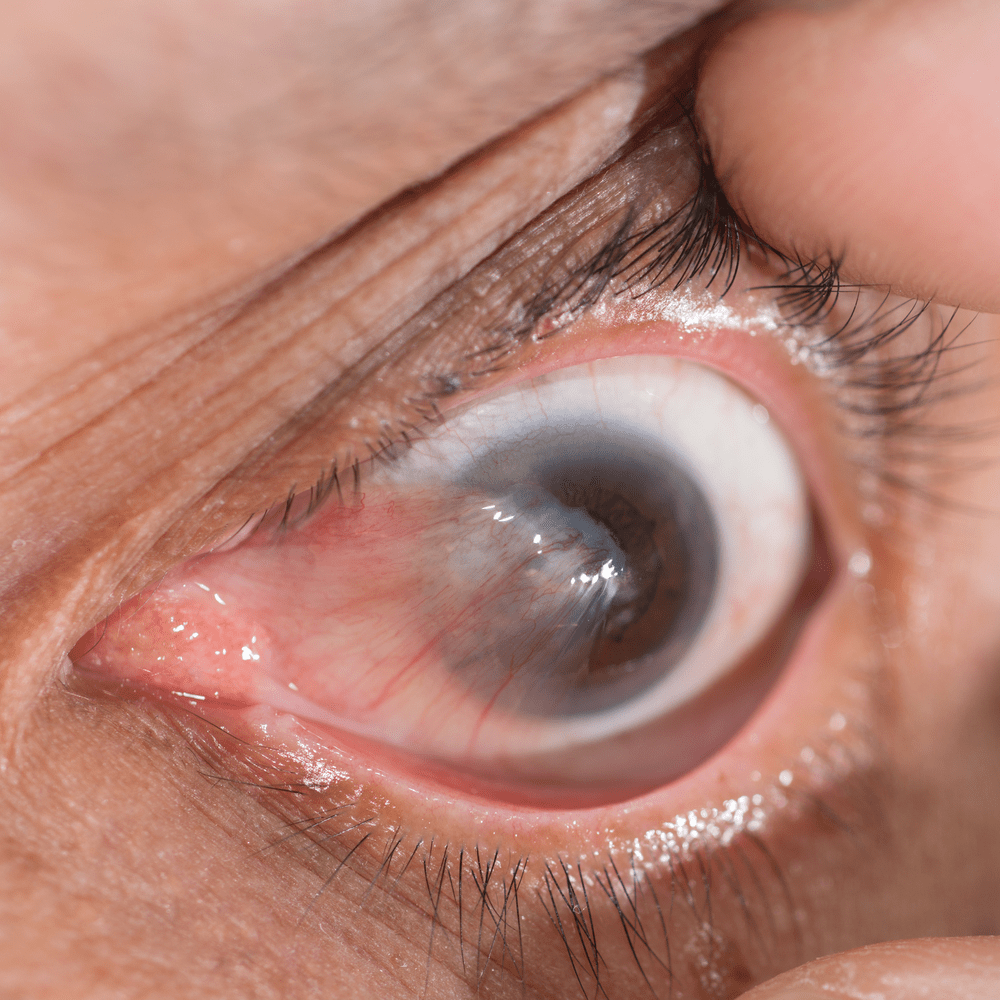
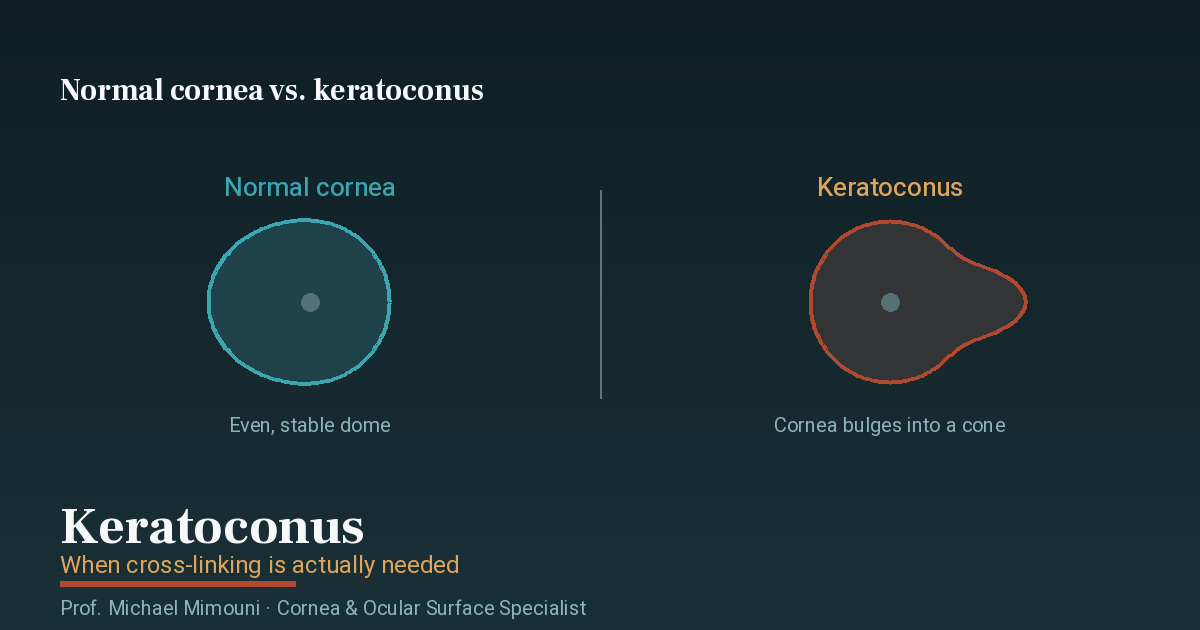
The cornea is the transparent “window” at the front of the eye — the dome through which light enters. In a normal eye it is dome-shaped and uniform, and its shape is what allows light to focus correctly on the retina. In keratoconus the cornea gradually weakens and thins, and instead of remaining a round, stable dome it is pushed forward and takes on a conical shape — hence the name “conical cornea.” The more the cone protrudes, the more irregularly light is refracted, and vision becomes blurred and distorted in a way that ordinary glasses struggle to correct.
The condition usually appears in adolescence or the early twenties, tends to progress during those years and gradually stabilises around midlife. It is almost always in both eyes, though usually to different degrees. The causes combine a genetic predisposition and mechanical sensitivity of the cornea — and vigorous, persistent eye rubbing, for instance on a background of allergy, is considered a factor that accelerates progression. This is one of the reasons I advise every patient with keratoconus to avoid rubbing their eyes and to treat allergy well.
The Symptoms That Raise Suspicion
In the early stages keratoconus can look like nothing more than “a prescription that keeps changing.” The things that raise my suspicion are:
- A glasses prescription that changes again and again, particularly a rapid increase in astigmatism (cylinder)
- Blurred or distorted vision that is not fully corrected with glasses
- Glare, halos around lights and night driving that becomes difficult
- The need to rub the eyes frequently
- A diagnosis of high astigmatism at a relatively young age
A definitive diagnosis is not made on symptoms alone but on computerised mapping of the cornea (topography or tomography), which shows the shape of the cornea and its thickness in detail. This examination is also what makes it possible to follow the condition over time and identify whether it is stable or progressing — and that distinction, as we shall see in a moment, is the heart of the treatment decision.
The Principle That Changes Everything: Stable vs. Progressing
The most important point on this page is this: the decision about cross-linking is not determined by how “severe” the keratoconus looks in a single examination, but by whether it is progressing. Stable keratoconus — one that does not change over time — can in many cases simply be monitored, with vision corrected by optical means, without any intervention in the cornea. Progressing keratoconus, by contrast, in which the cornea continues to weaken and change from examination to examination, is the situation in which cross-linking genuinely comes into the picture.
So when a patient arrives with a new diagnosis, my first question is not “whether to treat” but “is this progressing.” The answer comes from comparing examinations over time. In a young patient with clear signs of progression we will not wait long, because at a young age progression is faster and the opportunity to stabilise matters. In an older patient with a stable condition, monitoring alone may be the right thing. Both patients “have keratoconus” — but the recommendation for them is entirely different.
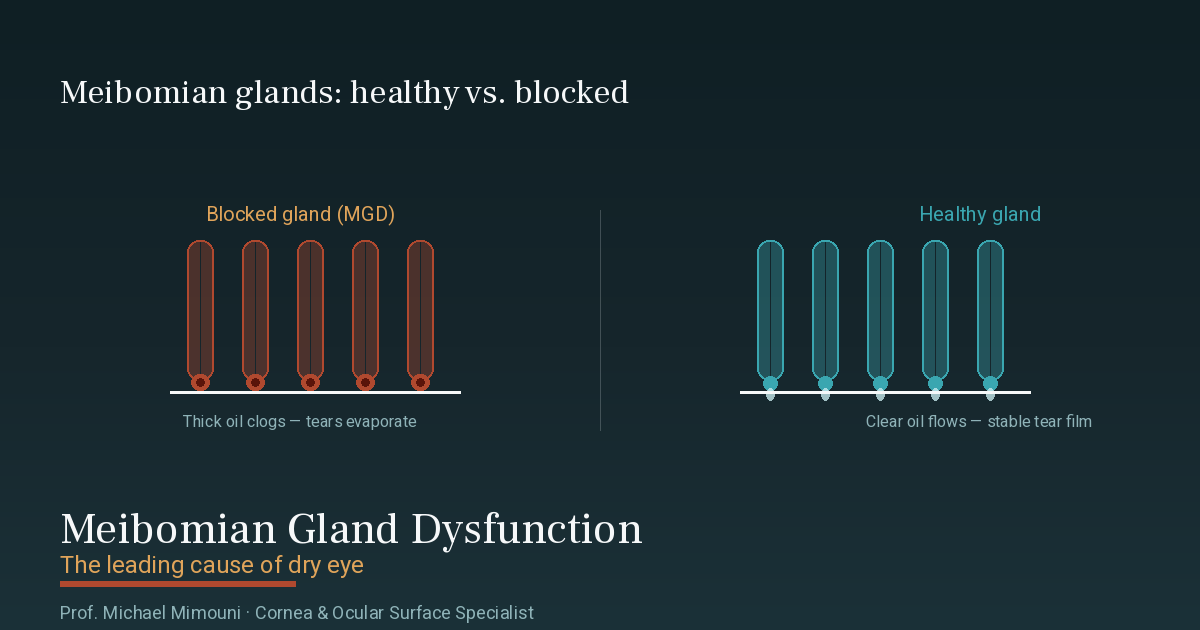
What Cross-Linking Does — and What It Does Not Do
Cross-linking is a treatment with a single aim: to strengthen the cornea and halt progression. In practice, vitamin B2 (riboflavin) is dripped into the eye and it is exposed to ultraviolet light (UV-A) at a controlled dose. The combination creates new bonds between the collagen fibres that make up the cornea — like reinforcing a net that has stretched — and the result is a stiffer, more stable cornea, far less inclined to continue deforming.
And here I want to be precise, because this is exactly the point at which there are many exaggerated promises. The goal of cross-linking is to halt progression, not to turn back the clock. The treatment stabilises the cornea and thereby prevents future deterioration — and often that is what spares a later decline to the point of needing a corneal transplant. What it generally does not do is cure the keratoconus, straighten a cone that has already formed, or give you back sharp vision without glasses or lenses. Sometimes a slight flattening of the cornea and some improvement are seen after the treatment, but this cannot be promised, and it is not the aim. Someone who approaches cross-linking expecting it to “fix their vision” may be disappointed; someone who approaches it in order to preserve what they have and prevent deterioration understands correctly what the treatment offers.
This is why I devote time to the expectations conversation before every treatment. Cross-linking is a good, well-established treatment when used at the right time and for the right reason — stabilising a progressing cornea. Honesty about what it does and does not do is part of good care.
Who the Treatment Suits — and Who It Suits Less
The treatment is suitable mainly for:
- Patients with proven progressing keratoconus, especially children, adolescents and young adults — the age group in which progression is faster
- Patients whose cornea is still thick and clear enough to undergo the treatment safely
- Situations where the aim is to preserve the cornea and prevent future deterioration
The treatment is less suitable, or requires separate consideration, in situations such as a very thin cornea (there is a minimum thickness considered safe for treatment), advanced keratoconus with significant central scarring, or a stable condition with no signs of progression, in which monitoring may be preferable to intervention. At the other end of the scale, very advanced keratoconus in which vision can no longer be corrected with lenses — cross-linking will no longer solve it, and there options such as partial corneal transplantation arise. For exactly these reasons the decision is never automatic, but is made after a full assessment of the shape of the cornea, its thickness, the degree of progression and the state of vision.
How Vision Is Corrected — a Separate Story from Treating the Cornea
This is one of the points that most confuses patients, so I will say it explicitly: cross-linking treats the stability of the cornea, not visual acuity. Even after a successful treatment that has stabilised the cornea, vision still needs to be corrected — and that is a separate path, chosen according to the degree of keratoconus.
In mild stages, glasses or soft contact lenses may suffice. As the distortion grows, rigid gas-permeable (RGP) or scleral contact lenses usually give far better vision, because they create a smooth optical surface over the irregular cornea. In selected cases intrastromal rings can be added to improve the shape. The choice is made together, according to what gives you the best and most comfortable vision.
One more thing is very important to know: laser vision correction (LASIK) is not suitable for someone who has keratoconus. The laser thins the cornea, and in a cornea already weakened this may accelerate progression. If you considered laser vision correction and keratoconus was discovered, that is precisely why it was ruled out — and it is a critical fact that anyone considering laser vision correction should have checked in advance.
When to See a Cornea Specialist
It is worth seeing a cornea and ocular-surface specialist for an evaluation if:
- You have been diagnosed with keratoconus and want to know whether it is stable or progressing, and what that means for you
- Your prescription keeps changing, or your vision is blurred even with new glasses
- It concerns a child or adolescent with a fresh diagnosis — here timing matters especially
- You have been told you need cross-linking and want a second opinion before deciding
- You were turned down for laser surgery because of your corneal shape and want to understand why
I carry out these evaluations and treatments, including cross-linking and long-term monitoring, at my Haifa clinic, serving patients across northern Israel. Accurate diagnosis and structured follow-up are what make it possible to catch progression in time — and often, in fact, to spare unnecessary intervention.
If you have been diagnosed with keratoconus, or you are worried about it and want to know exactly where you stand, you are welcome to get in touch and schedule an evaluation at my Haifa clinic. We will start with precise mapping of the cornea, and from there build the right plan for you together — whether that is treatment or monitoring.
Frequently Asked Questions
Does cross-linking cure keratoconus? No. Cross-linking strengthens the cornea and halts the progression of keratoconus, but it does not cure it and does not flatten a cone that has already formed. The goal is to stabilise the cornea and prevent future deterioration, and in doing so often to prevent decline to the point of needing a corneal transplant. Vision itself is still corrected separately, with glasses or lenses.
Does everyone diagnosed with keratoconus need cross-linking? Not necessarily. The decision is determined by whether the keratoconus is progressing. A stable condition can in many cases simply be monitored, with vision corrected optically, whereas progressing keratoconus — especially in children and young people — is the situation in which treatment is genuinely needed to halt the deterioration. So the first thing to establish is whether the condition is stable or progressing, based on comparing examinations over time.
Is the treatment painful and how long is the recovery? During the treatment the eye is numbed with drops, so it is not painful. The discomfort comes mainly in the first few days afterwards, when you may experience a foreign-body sensation, light sensitivity and watering while the outer layer of the cornea heals. Initial recovery usually takes a few days, and full stabilisation takes weeks. We go over the preparation and recovery details together before the treatment.
I have keratoconus — can I have laser vision correction? No. Laser surgery thins the cornea, and in a cornea already weakened by keratoconus this may accelerate the progression, so it is ruled out. If you were turned down for laser because of your corneal shape, this is usually the reason. Vision in keratoconus is corrected by other means — suitable glasses and lenses — not with laser.
Keratoconus and the military profile — what is important to know? Keratoconus is considered a medical condition that can affect vision classification at enlistment, and the details vary according to the individual situation and the degree of keratoconus. Beyond the military aspect, what matters most is to diagnose the condition, determine whether it is progressing, and treat or monitor accordingly — because those are what will affect your vision throughout life, far beyond the years of service.